

Brain. 2015;138(8):2120-2122.
Intraneuronal Lewy bodies and Lewy neurites consisting of aggregated α-synuclein (SNCA) are the hallmark of brain pathology in Parkinson's disease. It is now well established that Lewy-type α-synuclein histopathology also occurs in the peripheral autonomic nervous system (Beach et al., 2010; Gelpi, 2014), and recent efforts have been directed towards detection of this pathology in peripheral tissues in the hope that it could serve as diagnostic biomarker of Parkinson's disease. Such a tissue marker would differentiate Parkinson's disease from mimics and related conditions such as multiple system atrophy (MSA), essential tremor and vascular parkinsonism, which are not associated with Lewy-type α-synucleinopathy. In this issue of Brain, Zange et al. present the results of one such study on peripheral SNCA, and report the presence of phosphorylated α-synuclein (pSNCA) deposits in the dermal nerves of patients with Parkinson's disease, but not MSA or essential tremor, consistent with what one might expect from the known pathology of these disorders (Zange et al., 2015). The results thus suggest that a simple forearm skin biopsy could permit the separation of these conditions. Zange et al. also describe changes compatible with a neuropathy in their subjects with Parkinson's disease. As they observed a correlation between the pSNCA deposits and denervation of autonomic skin elements that was independent of age or disease duration, they suggest, as others have previously (Donadio et al., 2014), that pSNCA is causative for the nerve fibre degeneration. However, no conclusive evidence for this exists. The situation is similar to that in the CNS in Parkinson's disease, where it is unclear if Lewy bodies and neurites are causative factors, or bystanders of the neurodegenerative process.
Differentiating Parkinson's disease from MSA, particularly the so-called parkinsonian variant (MSA-p), can be difficult in clinical practice, especially in the early disease stages. Patients with MSA-p may respond well to levodopa and the usual red flags alerting for MSA may be missing. Ancillary tests can help in the diagnosis (Fanciulli and Wenning, 2015) but not uncommonly fail to solve the problem conclusively. Cardiac scintigraphy, for example, a test that has been found to correctly distinguish idiopathic Parkinson's disease with high sensitivity and specificity from MSA, was normal in a similar percentage of patients with Parkinson's disease and those with MSA (Zange et al., 2015).
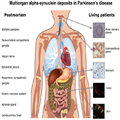
The search for peripheral SNCA deposits in living patients started with biopsies of the olfactory epithelium. Braak's elegant demonstration in post-mortem tissue of SNCA immunoreactive inclusions in the gastric wall of patients with Parkinson's disease (Braak et al., 2006) prompted studies looking for abnormal SNCA deposition in the gastrointestinal tract, and several studies have identified pSNCA in gastric and colonic specimens as well as in the salivary glands (Fig. 1; see Cersosimo and Benarroch, 2012 for a review).
The dermal nerves have also been the focus of studies in search of a peripheral SNCA marker. In post-mortem tissues, pSNCA has been detected in skin samples from the upper extremities, abdomen and scalp (Ikemura et al., 2008; Beach et al., 2010). In vivo studies assessing skin pSNCA deposits have reported on the presence of SNCA aggregates in patients with Parkinson's disease, with variable frequencies ranging from 0% to 100% (Wang et al., 2013; Donadio et al., 2014; Navarro-Otano et al., 2014), probably in part because different sites were selected for the skin biopsy. Zange et al. chose skin tissue obtained from punch biopsies from the forearm for their study and found SNCA aggregates in all 10 of their patients with Parkinson's disease, but in none of the patients with MSA or essential tremor.
The results of Zange et al. look promising but cannot be considered definitive, and previous studies with peripheral nervous system SNCA in Parkinson's disease suggest caution. Initial studies of colonic SNCA, for example, suggested that pSNCA deposits were highly specific for Parkinson's disease, but a recent study provides evidence for the presence of aggregated pSNCA in individuals with, as well as without Parkinson's disease (Visanji et al., 2015), suggesting that colonic deposition of pSNCA is not a useful diagnostic test.
Before we can consider ordering a skin SNCA study for diagnostic purposes, some important methodological issues need to be solved. The optimal site for study, for example, needs to be determined. We and others (Miki et al., 2010; Navarro-Otano et al., 2014) have failed to find pSNCA deposits in skin from the supramalleolar region and current evidence suggests that the highest yield may occur in skin tissue obtained in the cervical region (Donadio et al., 2014). Zange et al. promote the ventral forearm as the optimal site based on the assumption that there is a higher sweat gland density in this specific area. The issue is not quite settled and it remains possible that in Parkinson's disease the positivity for pSNCA in a given skin tissue also varies depending on disease stage, with distal regions more likely to have SNCA aggregates in very early stages, but perhaps less so later in the disease course. A centripetal propagation of axonal SNCA aggregates has been found to occur in the peripheral autonomic nervous system (Orimo et al., 2008).
The number of biopsies needed to obtain an optimal result is also unclear. While most studies have performed only one biopsy per site, Donadio et al. obtained the highest sensitivity (100%) by analysing two cervical skin samples, whereas the analysis of only one sample yielded a lower positivity rate. They attributed this finding to the likely patchy deposition of peripheral pSNCA. The size of the biopsies has also varied in the reported studies—between 3 and 6 mm—and could influence the rate of positivity, since larger biopsies are likely to enhance the probability of detecting autonomic structures and pSNCA deposits. Finally, methods of tissue fixation, choice of antibodies for immunohistochemistry and criteria for considering a biopsy positive or negative for pSNCA have differed considerably from one study to the next and made it difficult to compare results. For instance, in studies with a sensitivity higher than 80%, such as those of Zange et al. and Donadio et al., the assessment of the SNCA deposits is quite different. In Zange and co-workers' study, the presence of SNCA deposits was assessed qualitatively and semiquantitatively, and the detection rate was defined as the percentage of antibody-positive skin elements (sweat glands, arrector pili muscles and arterial blood vessels) relative to all detected skin elements. In the study by Donadio et al., the pSNCA staining was assessed with a fluorescence microscope and was rated in each skin site as the percentage of autonomic structures or nerve bundles showing a positive staining.
Researchers need to arrive at a consensus on procedure standardization and on how to move forward with studies to determine the sensitivity and specificity of skin Lewy-type α-synucleinopathy as a diagnostic biomarker for Parkinson's disease. This would hopefully reduce the variability of the results obtained and make them comparable. Eventually, studies focusing on expression patterns of pSNCA in the peripheral autonomic nervous system in premotor Parkinson's disease would seem warranted. SNCA accumulation has already been identified in the gastrointestinal tract in premotor Parkinson's disease (Hilton et al., 2014). Prodromic skin studies could be undertaken in subjects with a higher than average risk of developing Parkinson's disease such as those with idiopathic REM sleep behaviour disorder or asymptomatic carriers of leucine-rich repeat kinase 2 (LRRK2) mutations. These would ideally be prospective cohort studies, in which multiple additional markers (clinical, biological and imaging) would be assessed and subjects followed long term to capture the evolution to clinically defined Parkinson's disease. A reliable premotor biomarker could allow treatment to begin earlier and facilitate the development of treatments to slow or even halt disease progression.
The study by Zange et al. provides evidence that skin SNCA assessment may reliably separate Parkinson's disease from MSA, with no overlap between the two conditions in positivity for pSNCA in dermal nerves. This biomarker study, centred on a disease-related protein, needs to be replicated in an independent cohort and with a larger number of cases, and preferably with blind rating of the immunohistochemistry sections. The results of the study suggest though that we may be getting closer to finding an inexpensive and non- or minimally invasive diagnostic tissue marker of Parkinson's disease. Such a marker would be useful for separating Parkinson's disease from MSA and other parkinsonisms not associated with Lewy-type histopathology, and may eventually be used for confirming the diagnosis of very early, or even prodromal, disease.
http://www.medscape.com/viewarticle/850685?src=wnl_edit_tpal
No comments:
Post a Comment