
Press release
Researchers from Imperial College London and Newcastle University believe they have found a potential new way to target cells of the brain affected by Parkinson's disease.
The new technique is relatively non-invasive and has worked to improve symptoms of the disease in rats.
"If you were to peer inside the PPN, it is like a jungle with a massive variety of nerve cells that behave differently and have different jobs to do," said Dr Ilse Pienaar, Honorary Lecturer in Neuroscience at Imperial College London
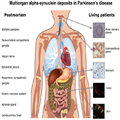
Scientists already suspect that cholinergic neuron cells are involved in Parkinson's disease. This is because in post mortem studies of patients? brains, about half of these cells have perished, for reasons that are currently unknown.
The researchers from Imperial College London and Newcastle University worked with rats that had been treated to recreate the symptoms of Parkinson's disease. They used a harmless virus to deliver a specially-designed genetic 'switch' to the cholinergic neurons. The rats were then given a drug that was designed to activate the 'switch' and stimulate the target neurons.
Following the treatment the rats made an almost complete recovery and were able to move normally.
Dr Pienaar adds: "This study confirms that cholinergic neurons are key to the gait problems and postural instability experienced by advanced Parkinson's disease patients. It also suggests that it's possible to target those cells that remain to compensate for those that are no longer functioning effectively, possibly due to weak communication between nerve cells. If we can transfer this technique into people, we believe this could help patients regain mobility.
"At the moment, neurosurgeons are attempting to target specific areas with deep brain stimulation, but it is a blunt tool with correspondingly mixed results. We think we have found a way to target only the cholinergic neurons within an area such as the PPN."
Dr Joanna Elson at the Institute of Genetic Medicine at Newcastle University added: "The structure we studied is complex, very complex. Despite this complexity and the intricacy of the techniques and the brain region analysed, the results are exciting because of the potential to advance patient treatment.
"This paper will help us understand how deep-brain stimulation works, but more importantly it is a step towards offering less invasive treatment options to patients with Parkinson's and other neurodegenerative disorders."
The researchers believe the technique could transfer into people in the next five to ten years. They also think their technique could have wider potential. Dr Pienaar said: "Parkinson's disease patients experience a complex set of symptoms and we hope to use the same method to understand how different cells within the brain contribute to the disease."
Dr Pienarr held a Junior Research Fellowship at Imperial during this work. She was also by the Rosetrees Trust and the British Pharmacological Society.
Pharmacogenetic stimulation of cholinergic pedunculopontine neurons reverses motor deficits in a rat model of Parkinson's disease, by Ilse S. Pienaar, Sarah E. Gartside, Puneet Sharma, Vincenzo De Paola, Sabine Gretenkord, Dominic Withers, Joanna L. Elson and David T. Dexter is published in Molecular Neurodegeneration on 23 September 2015, DOI: 10.1186/s13024-015-0044-5
Background
About Imperial College London
Imperial College London is one of the world's leading universities. The College's 14,000 students and 7,500 staff are expanding the frontiers of knowledge in science, medicine, engineering and business, and translating their discoveries into benefits for society.
Founded in 1907, Imperial builds on a distinguished past - having pioneered penicillin, holography and fibre optics - to shape the future. Imperial researchers work across disciplines to improve global health, tackle climate change, develop sustainable energy technology and address security challenges. This blend of academic excellence and its real-world application feeds into Imperial's exceptional learning environment, where students participate in research to push the limits of their degrees.
Imperial nurtures a dynamic enterprise culture, where collaborations with industrial, healthcare and international partners are the norm. In 2007, Imperial College London and Imperial College Healthcare NHS Trust formed the UK's first Academic Health Science Centre. This unique partnership aims to improve the quality of life of patients and populations by taking new discoveries and translating them into new therapies as quickly as possible.
Imperial has nine London campuses, including its White City Campus: a 25 acre research and innovation centre in west London. At White City, researchers, businesses and higher education partners are co-locating to create value from ideas on a global scale.
Key Facts:
- Newcastle University is a Russell Group University
- Ranked in the top 1% of universities in the world (QS World University Rankings 2014)
- Ranked 16th in the UK for global research power (REF 2014)
- Ranked 10th overall in the UK and 3rd for quality of staff/lecturers in the Times Higher Education Student Experience Survey 2015
- Winner: Outstanding Leadership and Management Team and Outstanding Procurement Team, Times Higher Leadership and Management Awards 2015
- Amongst our peers Newcastle is:
- Joint 6th in the UK for student satisfaction
- Ranked 1st in the UK for Computing Science research impact, 3rd in the UK for Civil Engineering research power and 11th in the UK for Mathematical Sciences research (REF 2014)
- Ranked 8th in the UK for Medical and Life Sciences research quality (REF 2014)
- Ranked 3rd in the UK for English, and in the top 12 for Geography, Architecture and Planning, and Cultural and Media Studies research quality (REF 2014)
- Engineering and Physical Sciences Research Council (EPSRC) top 20 strategic partner
- 94% of our students are in a job or further training within six months of graduating
- We have a world-class reputation for research excellence and are spearheading three major societal challenges that have a significant impact on global society. These themes are: Ageing, Sustainability, and Social Renewal
- Newcastle University is the first UK university to establish a fully owned international branch campus for medicine at its NUMed Campus in Malaysia which opened in 2011
- 90% Satisfaction level from our international students (ISB 2014)
- Newcastle University Business School is one of 20 Triple Accredited Business Schools in the UK
Contacts
For more information please contact:
Hayley Dunning
Research Media Officer
Imperial College London
e-mail: h.dunning@imperial.ac.uk
Tel: +44 (0)20 7594 2412
Research Media Officer
Imperial College London
e-mail: h.dunning@imperial.ac.uk
Tel: +44 (0)20 7594 2412
Kerry Noble
News Editor
Imperial College London
Tel: +44 (0)20 7594 3415
e-mail: k.noble@imperial.ac.uk
Out of hours duty press officer: +44(0)7803 886 248
News Editor
Imperial College London
Tel: +44 (0)20 7594 3415
e-mail: k.noble@imperial.ac.uk
Out of hours duty press officer: +44(0)7803 886 248



![[Neurons]](http://cdn1.medicalnewstoday.com/content/images/articles/299/299893/neurons.jpg)

